Household sanitation is a longstanding development priority for the government of Uganda. There has been a significant reduction in open defecation (from 12% in 2000 to 7% in 20151). However, access to basic sanitation2 is still low (19% in 20151) and the country is off-track to meet the Sustainability Development Goal related to universal access to sanitation by 2030. This, coupled with the government’s policy that considers sanitation to be a household responsibility,3 provides tremendous opportunity to foster market-based sanitation (MBS) as the mechanism to increase basic sanitation across the country.
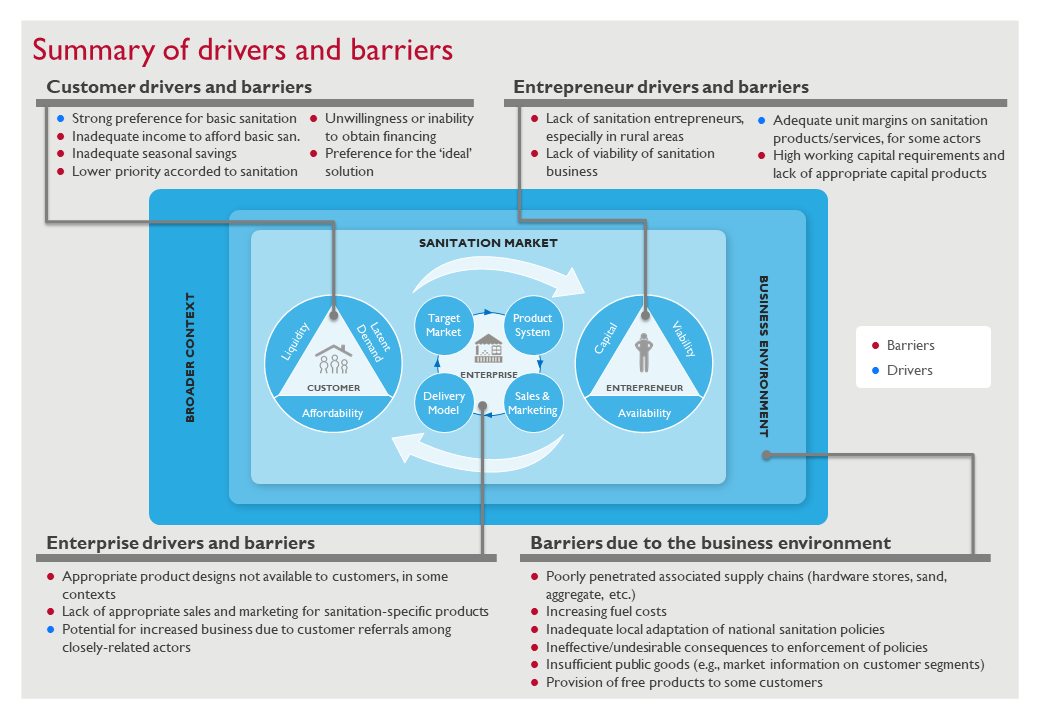
In 2018, FSG began working with the Uganda Sanitation for Health Activity (USHA)—a five-year program funded by the United States Agency for International Development (USAID)—to design and implement novel approaches to increase access to basic sanitation. As a part of this exercise, the FSG team identified drivers and barriers for the uptake of basic sanitation in Uganda, along the WASHPaLS framework for Scaling Market Based-Sanitation (MBS)4—see Figure 1 for a summary of these drivers and barriers. Based on these insights and further analysis, FSG supported USHA to develop the National Sanitation Market Guidelines for Basic Sanitation in Uganda (NSMG5), a strategic roadmap directing stakeholders on how to use MBS principles to increase access to basic sanitation services.
Figure 1: Drivers and Barriers to Uptake of Basic Sanitation in Uganda
In mid-2019, USHA leveraged the recommendations and insights from the NSMG to design an MBS model which is currently being piloted. The model is geared towards an appropriate target market, includes best-fit products for the target market, sales and marketing strategies to activate demand, and a delivery model suitable to prevailing market factors. This blog describes these four aspects of the model.
1. Selecting a Target Market
No two customers are identical, but groups of customers possess similar traits and show similar patterns related to their buying behaviors and preferences. Thinking about customers in a segmented manner helps actors develop and implement interventions in a targeted and tailored manner, leading to greater impact.
The NSMG provides findings from a detailed customer segmentation analysis conducted by FSG, and identified 11 customer segments: Segment A–Segment K (please refer to this blog for additional details). However, each segment is not equally amenable to MBS interventions. Among other reasons, some segments are not large enough to attract private sector participation, and some segments have low ability to pay. Accordingly, the NSMG suggests four priority segments for MBS, in the current market scenario.
Given the geographic overlap with its program activities in 2019, USHA chose two of these four segments (C and E) to begin with. The insights from the detailed segmentation analysis in the NSMG enabled USHA to design an enterprise model that was suitable to these segments’ needs and preferences.
2. Developing Best-Fit Products
FSG’s research suggests that sanitation products (i.e. toilet models) available in the market are either unaffordable or undesirable to many households within segments C and E. For example, Segment E has a median ability to pay of USD 144 (compared to USD 190 for segment C) while the typical price of the most common single stance improved toilet was about USD 210. Despite the lower ability to pay, households in Segment E want a durable, well-ventilated toilet that is safe for children and the elderly. Therefore, USHA needed to design best-fit products that strike an optimal balance between meeting customer preferences and needs, and their ability to pay. Given the variability in affordability and existing sanitation levels within a segment, a single product offering would not be affordable and attractive to all households within a segment. And so, USHA developed three product categories (base product, upgrade product, and new single or double stance product) to cater to a wider number of households within each segment.
USHA has designed a base product that includes a toilet pit and a durable toilet floor (or interface) made of cement, and thereby, safe for children and the elderly. The product also includes a ventilation pipe, and other options to help reduce smell in the toilet. While the base product includes features most important to the segment, it allows flexibility for households to build their superstructure (walls and roof) with the materials they desire, and over a time period that works better for them. This reduces the need for the households to make all investments up-front, and allows better affordability (USD 70–140 depending on the depth of the pit) while also meeting many of the customers’ preferences.
To cater to the lowest-income customers, and recognizing that most households in both segments already have a toilet, USHA designed a product that allows households with a sturdy but otherwise unimproved toilet to improve just the interface. By retrofitting a part of the existing unimproved toilet’s floor with a cemented floor, households can benefit from a more durable toilet that is safer and more hygienic to use at a more affordable price tag (about USD 27). USHA has developed this product for households that cannot afford to construct a new toilet, and for those that may have only recently constructed a new unimproved toilet.
A sizeable portion of Segment E—about 27%—can afford a toilet costing USD 160–240, and about another 10% can afford a toilet between USD 240–400. These households, with a higher ability to pay and a preference for double stance toilets, may want to invest in an even more feature-rich product, similar to the more commonly found single and double-stance improved toilets. USHA has optimized the design and material requirements of these common products. Thereby, an improved single-stance toilet can now be offered at a starting price of about USD 168.
3. Activating Demand
Many households interested in toilet construction (~60% of households in Segment E) put off their investment due to competing priorities or a lack of awareness of the best-fit products and pricing. Activating demand through door-to-door sales and marketing efforts, using messages tailored to the target segment, can be effective in dealing with this barrier. However, it is important to select the right demand activators.
The NSMG recommends that demand activators be persuasive, persistent, trustworthy, and have access to community networks. Thus, in most communities, USHA partners with village-based community health workers (known as Village Health Teams (VHTs)) to conduct door-to-door sales and marketing. To ensure that they remained incentivized, USHA encourages sanitation entrepreneurs to pay the demand activators a small commission for every successful lead (see next section for more details).
In addition to segments' affordability and product preferences, the NSMG also provides insight into each segment's beliefs related to sanitation. For example, Segment E greatly values the health benefits of toilets and their role in reducing disease and keeping families healthy—more so than other segments. In contrast, Segment C strongly values products used in urban centers, and aspires to make such lifestyle improvements. Keeping this in mind, USHA trained the demand activators on sharing specific messages that would better resonate with potential customers. For example, the sales pitch tailored to Segment E includes the following: “The toilet I am selling to you can be fitted with a ventilation pipe to make sure it does not smell. It will guarantee a high level of hygiene and ensure that your family is protected from disease.”
Before the activators commenced door-to-door marketing in the pilot communities, USHA conducts a community-wide triggering session to encourage households to adopt basic sanitation. Unlike traditional triggering sessions6 that focus on shame—such as naming households that defecate in the open, conducting a walk of shame to open defecation areas—the triggering sessions designed by USHA focus on providing households with an overview of the products, reinstating relevant messages related to family pride and health, and introducing households to the relevant actors (activators and sanitation entrepreneurs) in their community.
4. Facilitating an Appropriate Delivery Model
Households constructing an improved toilet in Uganda typically interact with as many as eight material and service providers. The prevailing do-it-yourself delivery makes it difficult for households to identify the product best suited for themselves, or to easily obtain information on the construction process and materials required. The process is inconvenient, lengthy, and expensive, and leads to variable product quality. Introducing a sanitation entrepreneur in the market can streamline the process and help solve some of these challenges.
As suggested by the NSMG, a sanitation entrepreneur should be easily accessible to customers, make healthy margins on toilet constructions, be motivated to grow the sanitation business, and have basic construction skills. Keeping this in mind, USHA chose masons as the sanitation entrepreneurs for segments C and E. Prevailing market dynamics and barriers have dictated the role of the mason. For example, USHA expects masons, and not activators, to provide households with information on where to buy materials, since most masons already know the local material suppliers. Further, USHA does not expect masons to purchase materials on behalf of the household, as masons have limited access to working capital financing, and may also not be adequately trusted by households to do so. Households’ lack of trust towards masons is another reason USHA does not encourage masons to purchase materials. Thus, USHA developed a network delivery model, with the mason playing the role of aggregating information and constructing the toilet.
USHA has identified and trained interested masons in the community and linked them to the demand activators. Once an activator generates a lead, the mason is responsible for meeting the customer and confirming the product most suited for them. The mason provides the household with a bill of quantities that lists materials required, their associated prices, and recommended local suppliers. This aggregated information sharing is key to the network delivery model, as it can help make the construction process more transparent, easier, and cheaper for the household.
The model described above was developed between March and August 2019. Since August 2019, USHA has been piloting the model in select locations within 13 districts in Uganda. FSG continues to support implementation and to iterate on the model based on field learnings.
We look forward to sharing more insights regarding implementation learnings, early impact, and additional interventions (if any) in subsequent blogs.
Acknowledgement: The NSMG was developed by FSG with support from USHA. From FSG, Akshay Kohli, Anantya Chandra, Anindita Ravikumar, Jaagruti Didwania, Meghana Puri, Puneet Goenka, Rahul Singh, Rishi Agarwal, and Vignesh Shankar contributed to the underlying research and development of the NSMG.
1 The Uganda National Household Survey 2016-2017.
2 Refer to the sanitation ladder by the Joint Monitoring Programme for Water Supply and Sanitation by WHO and UNICEF to understand the different sanitation levels.
3 Direct government or donor investment is generally unavailable to households.
4 For a detailed explanation of the framework, refer to Scaling Market Based Sanitation: Desk review on market based rural sanitation development programs, Agarwal R., Chennuri S., and Mihaly A., USAID Water, Sanitation, and Hygiene Partnerships and Learning for Sustainability (WASHPaLS) Project, Washington, DC., June 2018.
5 The NSMG is currently under review, and awaiting endorsement from Uganda’s Ministry of Health
6 Triggering sessions are an important aspect of Community-Led Total Sanitation (CLTS), an approach used mainly in developing countries to improve sanitation and hygiene practices by ending open defecation.